To some degree, all programs serving struggling teens are grappling with the issues of Evidence-Based Practice or Best Practice. The reason: There is an emerging mandate in the mental health practice for a scientific basis in treatment. Stakeholders are beginning to demand it. Parents and referral sources are asking, "Does it work?" or "Why do you use that approach?" And they should. The problem is that the revolution seems so onerous and perhaps "at odds" with what we hold dear -- the "magic" or creativity of therapy. However, I believe the emerging model and resources of Evidence-Based Practice make it more inviting than it had been in the past and more readily viewed as a fundamental part of Best Practice.
Perhaps the best way to describe the emerging Evidence-Based Practice model within Best Practice is to define the key terms and their interrelationships. These terms are used inconsistently, causing confusion and resulting, I believe, in a "bad rap" for Evidence-Based Practice.
Empirically Supported Treatment (EST): EST is narrow term, referring exclusively to the use of treatments where there is strong scientific support of effectiveness. The source of EST is scientific evidence gathered by an infrastructure charged with the task of conducting, evaluating and disseminating research on treatments. ESTs are available for adolescents with internalizing conditions (anxiety and depression), externalizing conditions (aggression, defiance and disruptive behavior), chronic mental illness and substance use problems. Some levels-of-care are probably too multi-faceted to evaluate as an EST, such as outpatient, inpatient, wilderness and residential therapy. Instead, the treatment approaches used (functional family therapy) at a level of care are the point at which we find ESTs.
The tricky part for caregivers seems to be identifying which treatments qualify as ESTs. Fortunately, a new EST infrastructure does that for us and makes it readily available. It is important to remember that one published research article, or even a dozen published research articles, does not qualify a treatment as an EST. In fact, the infrastructure uses a complex process to make the EST designation, which typically involves screening thousands of research studies according to an elaborate set of criteria. The following organizations and websites provide "Gold Standard" listings of ESTs:
Each website contains authoritative lists of ESTs, with a wealth of easy-to-digest information. The good news is these lists contain only those treatments that have shown effectiveness in research conducted in "real" clinical settings, not just university laboratories. I recommend looking at the websites. The time is coming - or has come - when every viable program will be expected to have a "tool box" filled with ESTs. Fortunately, many of the ESTs are portable, affordable and applicable to our programs, students and families (parent training, drug prevention training, social skills training).
It is important to note that EST has limitations. There simply are not enough ESTs to meet the diverse needs of our students and families. Of the 200 mental disorders listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2000) applicable to youth, only a minority have treatments for which there is a strong evidence-base (none for reactive attachment disorder in teenagers). It takes about 15 to 20 years for a treatment to funnel thru the EST appraisal filter. Yet, our clients need services now. This means we need another component in the Evidence-Based Practice model of Best Practice: Clinical Consensus.
Clinical Consensus: Consensus is typically derived from a widely held standard of care, or guild guidelines, like those promulgated by NATSAP, OBHIC and IECA. Many experts consider clinical consensus and guild guides to be a "nonscientific source of evidence," but types of evidence nonetheless (Drake, Merrrens, & Lynde, 2005, Norcross, Beutler, & Levant, 2006).
Often, ESTs are created "in the trenches" by the caregivers. Caregivers innovate to meet the changing and diverse needs of students and families. Through that process, new ways of helping start to emerge. For example, clinical consensus places high value on experiential therapies (art, music and equine) for struggling teens. Sufficient research is not available to evaluate experiential treatments as ESTs for our student population. However, until the research is completed, it is responsive and innovative for our programs to use them. In doing so, the caregivers simultaneously meet clinical needs and alert researchers to a treatment meriting scientific evaluation.
Outcome Research: Outcome research is now vital at every level-of-care in the mental health industry. Outcome studies have many benefits, including the obvious, such as evidence of effectiveness, and the not so obvious, such as defining admission/ discharge criteria, program improvement and marketing. Satisfaction surveys or "feedback" surveys, though meaningful aspects of an outcome study, do not become an outcome study, per se. The essential component of a mental health outcome study is a measure of client psychosocial functioning, whether it is in a survey, interview, or a behavioral rating scale. Our industry suffers from a dearth of outcome research that uses quality, standardized outcome measure, and quickly needs to move in that direction for its outcome research to be viewed as reliable or valid.
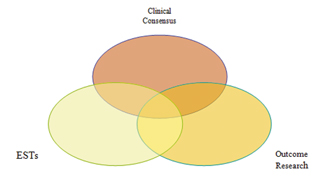
Evidence-Based Practice: In the emerging model, Evidence-Based Practice requires the strategic use of aforementioned components: ESTs, Clinical Consensus and Outcome Research. Specifically, an Evidence-Based Practice model places the ultimate authority in the category of Clinical Consensus. Yes, we should use ESTs when they "fit" the program, youth and families, but ESTs never take priority over the collective judgment of the experts in the trenches. If Clinical Consensus indicates that a particular EST seems inappropriate, then, according to the model, it is. Last, in this model, outcome studies are a "business-as-usual" practice. The purpose being a routine measurement of the youths' functioning after leaving a program - given the unique combination of the ESTs, the Clinical Consensus and everything else that make it up.
Evidence-Based Practice is a flexible model. It is not a manualized treatment applied the same way to all people. It promotes the use of treatments for which we have the best research support. When there are not ESTs that "fit," we use our collective wisdom to find innovative ways to help. Evidence-Based Practice is also a creative model. It places high value on the generative, creative role of the caregivers who are most aware of the needs of students and families. It creates a flow of information about promising treatments from the caregivers to the researchers. Last, Evidence-Based Practice is a responsible model. It raises the bar of accountability to a higher level - requiring us to study our outcomes and learn from them. Its systematic blend of science and collective wisdom allows us to be both responsible as an industry and responsive to our students and families.
Components of Evidence-Based Practice
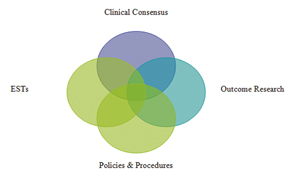
Best Practice: Evidence-Based Practice is often used as a synonym for Best Practice. Indeed, both concepts involve a careful blending of ESTs, Clinical Consensus and Outcome Research. However, when experts refer to Best Practice they typically include another component: Program policies and procedures - P & Ps. For example, admissions practices or human resource policies may qualify as P & P Best Practices. Many of the P & P Best Practices are not amenable to empirical validation and do not rely on clinical consensus. Nonetheless, they are important to the delivery of quality services. For the sake of clarity, it seems most precise to use the circumscribed term, Evidence-Based Practice, when referring to treatment interventions or approaches.
Components of Best Practice
So, where does this lead? I believe Evidence-Based Practice is necessary and good, as currently conceptualized. It will support our efforts to give the best to youth and families. However, how much are we doing about Evidence-Based Practice in our industry? Are we using it as a fundamental component of Best Practice? I think we need to do more. Specifically, I think we need to do systematic research on our outcomes. Why not come together to systematically research our services through partnerships, consortiums or work groups. Why not pass our ESTs and "treatments of clinical consensus" through evidentiary filters? Most other sectors within mental health service delivery are already doing that. Granted, there are limitations with the scientific process that are likely to create tension. Nevertheless, if we do not spearhead our own inquiry process, what will we say to our families and referring professionals about the effectiveness of our services? OBHIC has taken a lead on this issue. In addition, Dr. John Santa is convening a Research Summit thru NATSAP. Possibly efforts such as these can move our industry closer to an evidence-based, best practice model. Let's work together to make it happen.
References: Drake, R.E., Merrens, M.R., & Lynde, D.W (Eds.). (2005). Evidence-based mental health practice: A textbook. New York: Norton.
Kazdin, A.E. & Weisz, J.R. (Eds.). (2003). Evidence-based psychotherapies for children and adolescents. New York: Guilford.
Norcross, J.C., Beutler, L.E., & Levant, R.F. (Eds.). (2006). Evidence-based practices in mental health: Debate and dialogue on the fundamental questions. Washington DC: APA.
About the Author:
Ellen Behrens, PhD is a Licensed Psychologist and owner of Canyon Research and Consulting, a company that provides consulting and training services to mental health treatment programs and providers. She has extensive experience working in residential programs as a clinical director, psychological evaluator, therapist, researcher and consultant.
~Comments~
May 07, 2006
Thank you for delineating the subject matter so well. I was talking to Larry Stednitz about logical (common sensical) best practices in opposition to emperical tested practices (scientific). Safety First is an obvious best practice but where does it fit? Discipline/Care/Trustworthiness results in a trusting relationship. If you don't develop a trusting relationship with our clients, they won't feel safe or secure enought to do the tough work needed in a treatment program for emotionally disturbed youth. Having a set of basic human needs which could come under the Clinical Consensus umbrella might qualify as logical best practices....i.e. taking these into account in the individual treatment planning. An interesting area. Thanks again for the structure for thinging about these issues.